OphReason-Vision
15,418 reasoning trajectories synthesized from 100K+ clinical cases and 30+ public datasets, with expert agreement κ = 0.82.
A 2B-parameter vision-language model that learns clinical reasoning in the order clinicians do: from visual perception to integrated diagnostic judgment.
School of Artificial Intelligence and Automation, Huazhong University of Science and Technology · * Corresponding author
Ophthalmic MLLMs are constrained by unstructured training data, flat training strategies, and model sizes that limit practical deployment. OphVLM-R1 closes the loop across data, model, and optimization.
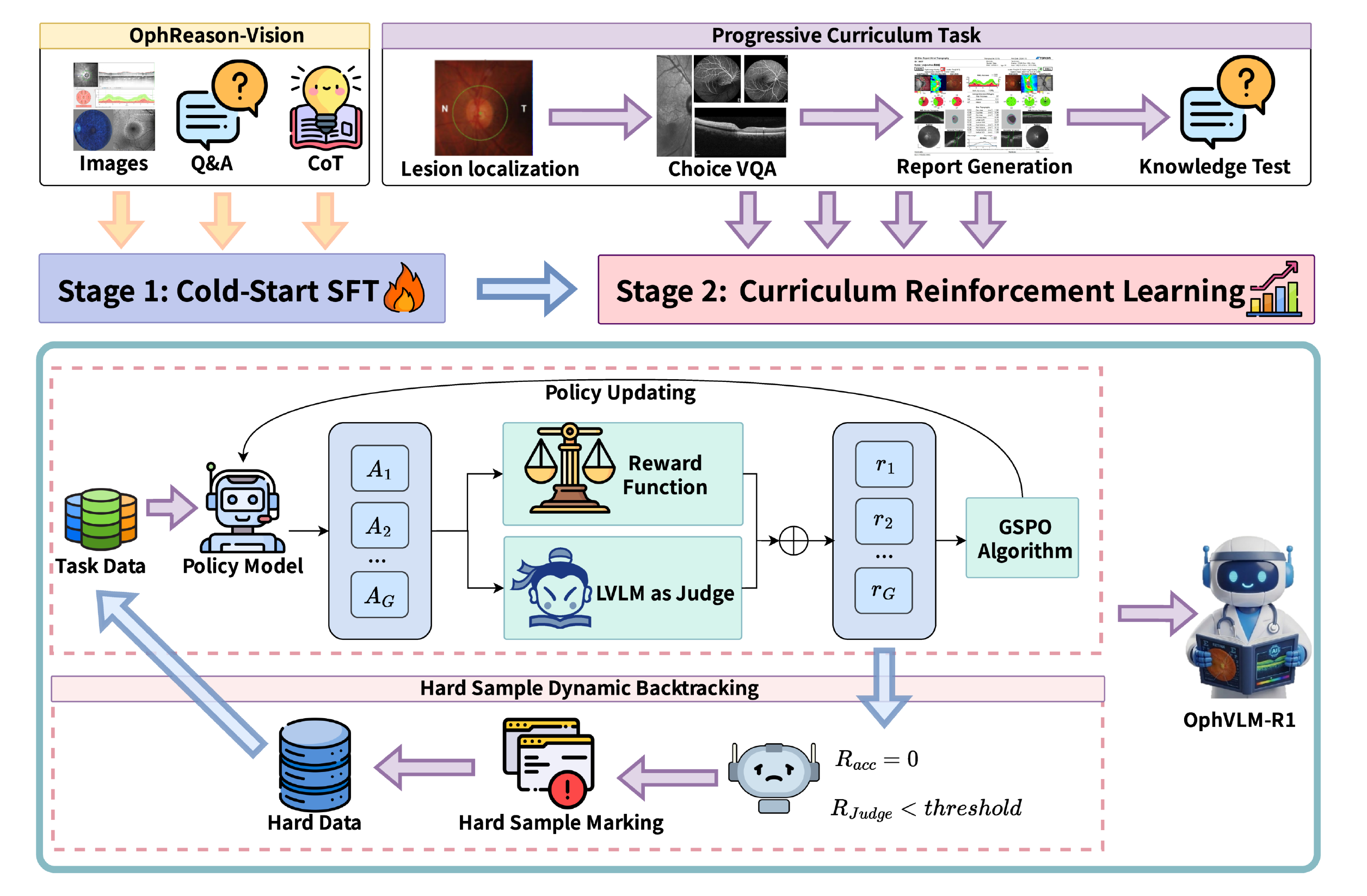
The pipeline combines verified Chain-of-Thought data, LoRA-based supervised fine-tuning, and curriculum reinforcement learning with sequence-level optimization and hard-sample dynamic backtracking.
15,418 reasoning trajectories synthesized from 100K+ clinical cases and 30+ public datasets, with expert agreement κ = 0.82.
Sequence-level policy ratios reduce variance accumulation across long clinical reasoning chains.
Persistently failed prompts return with higher sampling probability while keeping every rollout on-policy.
Four tasks increase in diagnostic complexity and follow the clinical workflow from perceptual grounding to knowledge-intensive decisions.
Single-image visual grounding
Cross-image diagnostic evidence
Structured long-form reasoning
Visual findings + clinical knowledge
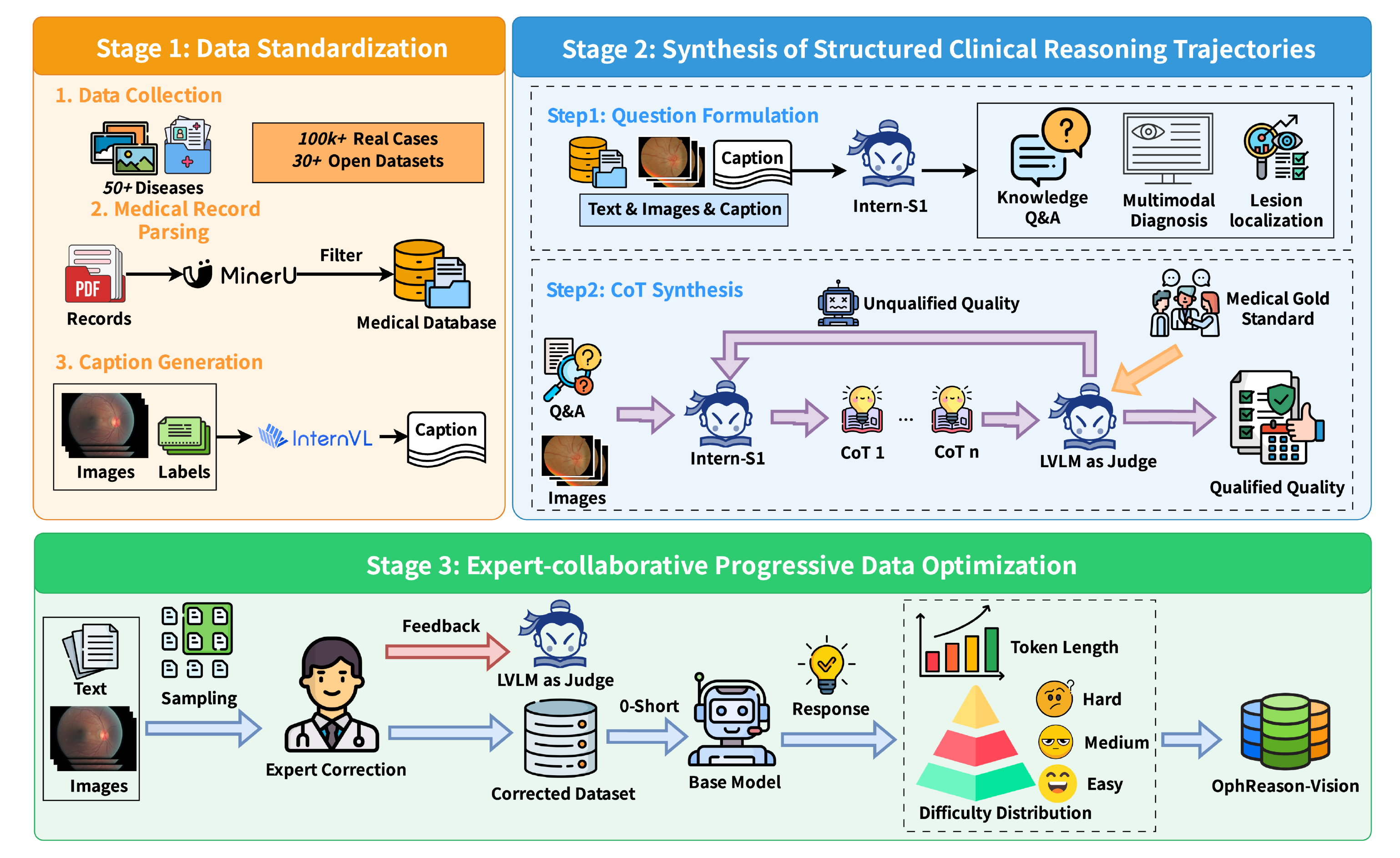
Standardization, structured synthesis, and expert-collaborative optimization turn heterogeneous ophthalmic records into quality-controlled reasoning trajectories.
13,418 training samples + 2,000 held-out cases
| Subset | N | Token range | Images | Purpose |
|---|---|---|---|---|
| cold_start | 3,418 | 1,609–2,113 | 1–2 | Cold-start SFT |
| Lesion Localization | 2,700 | 1,038–1,069 | 1 | Stage 1 |
| Multi-image Selection | 2,700 | 1,115–2,240 | 1–2 | Stage 2 |
| Report Generation | 3,600 | 1,012–5,985 | 1–5 | Stage 3 |
| Knowledge Q&A | 1,000 | 1,012–5,985 | 1–5 | Stage 4 |
| eval_in_domain | 2,000 | 1,060–1,138 | 1–2 | Evaluation |
OphVLM-R1 is evaluated on held-out in-domain cases, 31 fine-grained fundus tasks, and an out-of-domain ophthalmic VQA benchmark drawn from 11 independent sources.
Three complementary dimensions of ophthalmic reasoning
| Dataset | Samples | Tasks | Type |
|---|---|---|---|
| In-Domain | 2,000 | 4 | Multiple-choice |
| Fundus-MMBench | 620 | 31 | Fine-grained fundus |
| OmniMedVQA-Eye | 10,044 | 11 sources | Out-of-domain VQA |
Accuracy (%) · best and second-best are highlighted per benchmark
| Model | In-Domain | Fundus | Omni-Eye | Avg.* |
|---|---|---|---|---|
| Generic MLLMs | ||||
| InternVL3.5-2B | 34.50 | 36.61 | 55.47 | 42.19 |
| InternVL3.5-4B | 36.23 | 42.10 | 77.51 | 51.95 |
| Medical MLLMs (RLVR) | ||||
| MedVLM-R1-2B | 27.80 | 20.81 | 68.06 | 38.89 |
| Large medical MLLMs (SFT, off-the-shelf) | ||||
| Lingshu-7B | 44.20 | 41.29 | 87.42 | 57.64 |
| HuatuoGPT-Vision-7B | 38.30 | 28.06 | 71.78 | 46.05 |
| Ophthalmic MLLMs (SFT, off-the-shelf) | ||||
| FundusExpert-8B | 31.20 | 54.84 | 64.71 | 50.25 |
| Ophthalmic MLLMs (RLVR) | ||||
| OphthaReason-Intern-2B | 31.00 | 35.48 | 79.61 | 48.70 |
| OphthaReason-Qwen-3B | 36.60 | 38.87 | 86.86 | 54.11 |
| OphVLM-R1-2B (Ours) | 38.40 | 42.58 | 88.24 | 56.41 |
* The cross-benchmark average is reference-only because task scales, formats, and random baselines differ. Within-benchmark ranking is the meaningful comparison.
Ablation study · ΔOmni is the drop from the full model
| Configuration | In-Domain | Fundus | Omni-Eye | ΔOmni |
|---|---|---|---|---|
| OphVLM-R1 (Full) | 38.40% | 42.58% | 88.24% | — |
| Training strategy | ||||
| SFT Only | 37.52% | 34.47% | 62.03% | −26.21 |
| SFT + RL One-shot | 37.96% | 38.62% | 78.14% | −10.10 |
| SFT + RL Shuffled | 37.73% | 37.85% | 76.48% | −11.76 |
| Stage ablation | ||||
| w/o Stage 1 (Lesion Loc.) | 38.14% | 40.43% | 85.62% | −2.62 |
| w/o Stage 2 (Multi-image) | 38.02% | 40.17% | 85.13% | −3.11 |
| w/o Stage 3 (Report Gen.) | 37.88% | 39.72% | 84.38% | −3.86 |
| w/o Stage 4 (Knowledge QA) | 38.07% | 40.31% | 85.47% | −2.77 |
| Component ablation | ||||
| w/ GRPO (token-level) | 37.84% | 39.76% | 84.52% | −3.72 |
| w/o Hard Sample BT | 38.11% | 40.83% | 86.12% | −2.12 |
2B-parameter ophthalmic multimodal reasoning model.
Verified ophthalmic Chain-of-Thought reasoning trajectories.
Open-source code for the associated ophthalmic agent system.
If OphVLM-R1 or OphReason-Vision supports your research, please cite the WAICA 2026 paper.
@inproceedings{qi2026ophvlm,
title = {OphVLM-R1: Efficient Ophthalmic
Reasoning via Curriculum Reinforcement Learning},
author = {Qi, Zishi and Hu, Xiaoya and Pan, Huilin
and Gao, Ang and Hou, Jiaxin and Li, Jiankun
and Qian, Yongao},
booktitle = {Proceedings of the World Artificial
Intelligence Conference Academic (WAICA)},
year = {2026}
}